
[ad_1]
At a recent faculty meeting, my colleagues and I spent a considerable amount of time discussing how to improve our academic internal medicine clinic’s performance on hypertension clinical quality measures (CQMs), some of which were tied to financial incentives. Our discussions included plans to review reports and schedule return visits for patients with elevated in-office blood pressure readings, yet I questioned whether we were acting on the right data. Due to the many errors associated with in-office blood pressure measurement, clinical guidelines emphasize the importance of home blood pressure monitoring (HBPM) for the diagnosis and management of hypertension. However, the specifications for the CQMs that determined our performance did not allow for inclusion of most home blood pressure readings. We were working hard to improve our clinical quality measure performance, but I questioned whether we were actually improving quality.
Clinical Rationale And Guidelines For HBPM
The discrepancies between home and in-office blood pressure assessment have been noted since the 1940s. Patient-related factors leading to inaccurate measurement include acute meal ingestion, acute alcohol, caffeine, nicotine use, or bladder distention. Procedure-related factors include use of non-validated devices, improper positioning of the patient, incorrect cuff size, insufficient rest time, and talking during measurement. Finally, the “white-coat effect” can lead to elevated office blood pressure but normal home blood pressure.
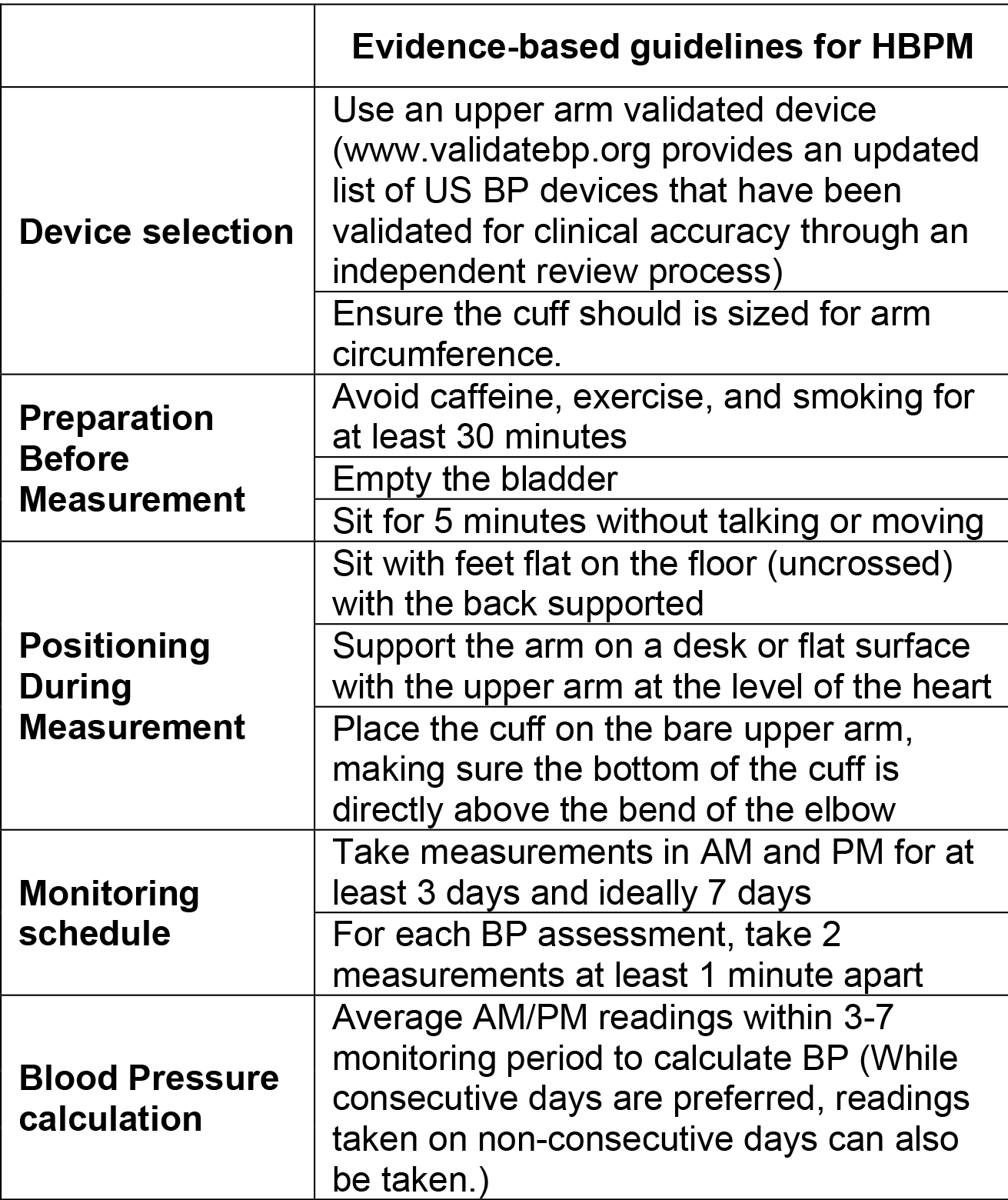
Increasing evidence suggests that systematic HBPM provides a more reliable assessment of blood pressure compared to in-office blood pressure. In 2008, a joint statement from the American Heart Association (AHA), the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association led by renowned hypertension expert Thomas Pickering, MD, called for HBPM to become “a routine component of blood pressure measurement in the majority of patients with known or suspected hypertension.” The European Society of Hypertension (ESH), the American Medical Association (AMA), and the Centers for Disease Control and Prevention (CDC) Million HeartsÒ Initiative all now strongly encourage HBPM. In 2021, the US Preventive Services Task Force reaffirmed its 2015 “Screening for High Blood Pressure in Adults” recommendation to obtain measurements outside of the clinical setting by either home or ambulatory monitoring for diagnostic confirmation of hypertension before starting treatment. To ensure accurate HBPM, the AHA, AMA, ESH, and CDC all offer similar guidance on device selection, technique, and monitoring schedule as summarized in exhibit 1.
Exhibit 1: Guidelines for home blood pressure monitoring

Source: AHA/AMA joint statement on self-measured blood pressure monitoring at home.
Barriers To Adoption Of Accurate HBPM
Despite more than a decade of guidelines calling for the adoption of HBPM, blood pressure continues to be measured at most office visits, and these potentially inaccurate readings continue to be those typically used for clinical decision making about hypertension. The uptake of evidence-based HBPM in the United States is low. Less than half of hypertensive adults engage in monthly or more HPBM of any kind, and only about one-third of hypertensive patients report being told by their doctor to do HPBM.
Unfortunately, CQMs and other policy regulations have been slow to incorporate approaches to promote evidence-based HBPM, likely contributing to low adoption. The Centers for Medicare and Medicaid Services (CMS) CQM, “Controlling High Blood Pressure,” which measures the proportion of hypertensive patients with a blood pressure less than 140/90 mmHg during the monitoring period, has only been amended in 2022 to include blood pressure measurements obtained by remote monitoring devices and conveyed to the clinician. While these modifications are a step in the right direction, at least in our internal medicine clinic, we have yet to adopt a workflow to incorporate HBPM readings into our quality performance data. Importantly, the CQM specifications also do not capture whether the measurement is obtained with a validated device or accept submission of an average home blood pressure despite HBPM guidelines recommending clinical decision making based on this calculation.
Remote patient-monitoring codes that have evolved over the past several years since they were introduced by CMS in 2017 are also based on policies that contradict guidelines. These codes are intended to incentivize clinicians to adopt remote monitoring, including HBPM. However, they require patients to transmit their blood pressure data to clinicians for at least 16 days per month, a criterion again inconsistent with guidelines for HBPM that call for three to seven days of measurements per month.
Another barrier to HBPM is the lack of widespread insurance coverage for blood pressure devices. A validated automated home blood pressure monitor costs between $30 and $100. In contrast to blood glucose monitors, Medicare does not typically cover upper arm blood pressure monitoring devices for routine HBPM with the exception of annual ambulatory blood pressure monitoring for patients with suspected masked or white coat hypertension. Few private payers and Medicaid plans provide coverage for HBPM.
Implementation Of Accurate HPBM
Despite its continued use, there is little utility for blood pressure measurement in the office for the diagnosis and management of hypertension. In my vision of evidence-based HPBM, in-lieu of in-office measurements, all patients should have access to a validated upper arm home blood pressure monitor with an appropriate cuff size, ideally covered by health insurance. Patients should be asked to perform occasional HBPM monitoring sessions, taking two readings one minute apart in the morning and evening for three to seven days. Providers or staff should provide patients with education about positioning and timing of the readings, including rest intervals. The provider should base clinical decisions on the average blood pressure of each three-to-seven-day monitoring period. CQMs should be amended to accept the submission of an averaged result, and remote monitoring platforms should easily be able to transmit this data to the electronic health record. Remote patient-monitoring incentives should require only three to seven days of monitoring.
There clearly is a need for improvement of blood pressure control in the United States. However, rather than spending our time reviewing reports of patients with elevated in-office measurements that are fraught with error, we should be educating our patients about how to conduct evidence-based HBPM to ensure that we are making clinical decisions based on accurate data. We should be advocating for payers to support these approaches rather than maintaining our antiquated status quo. As we continue to usher in an era in which provider payment is tied to value, we also need to remind ourselves that accurate data are a critical component to the provision of high-quality care.
Author’s Note
Dr. Litvin is vice president of research and innovation of the PPRNet Foundation, a nonprofit organization to promote evidence-based primary care. Dr. Litvin is co-founder of Stevara, LLC, a startup focused on developing technological solutions to improve the delivery of evidence-based health care including BPCorrect, a home blood pressure remote monitoring platform. Dr. Litvin would like to thank Dr. Steven Ornstein for his valuable feedback on this submission.
[ad_2]
Source link


{kind=link}