
[ad_1]
Many historically marginalized populations have faced differential access to COVID-19 resources, such as testing, vaccinations, or therapeutics. To date, national efforts to increase access to COVID-19 testing have included support for rural health clinics and local pharmacies, extending insurance coverage for at-home tests, and distributing free at-home tests directly to households. Yet, making tests available through existing health networks or online platforms does not remove all systemic barriers including limited access to reliable broadband access, low insurance coverage rates, or limited trust and access to primary care physicians or pharmacy networks.
Furthermore, data show persistent gaps in access and uptake of at-home COVID-19 test kits, noting usage most common among non-Hispanic, White adults, individuals ages 30–39, and individuals with household incomes above $150,000. Recent widespread rollback of measures that protect communities systemically excluded from health systems—including masking mandates and reductions in funding for COVID-19 mitigation services for populations who are uninsured—illustrate the need for continued efforts to provide equitable, community-based COVID-19 testing solutions for historically marginalized populations.
Systemic barriers will continue to be foundational in inequalities that we can anticipate in care for communities experiencing the greatest impact by subsequent COVID-19 waves, limited access to test-to-treat models, and postacute COVID-19 syndromes.
In September 2020, the National Institutes of Health (NIH) launched the Rapid Acceleration of Diagnostics-Underserved Populations (RADx-UP) initiative with a $500 million investment in community-engaged research. Its aim is to increase access and uptake of SARS-CoV-2 tests in historically marginalized populations. RADx-UP represents the single largest health disparities research investment in the history of the NIH.
More than 120 RADx-UP projects are evaluating community-based research studies to serve communities experiencing the greatest impact of COVID-19, including Black, Hispanic, Latino or Latinx, American Indian, Alaska Native, Asian, Native Hawaiian and Pacific Islanders communities as well as people who live in rural areas or are incarcerated, low-income, unhoused, older adults, children, disabled, and pregnant. The RADx-UP projects are evaluating strategies to remove barriers that prevent people from accessing testing in a timely manner—a necessary step for ongoing access to COVID-19 treatment and broader health reform efforts to improve population health.
Community-based COVID-19 testing models offer a solution to redress historical and contemporary experiences of systemic exclusion and structural racism that contribute to adverse health outcomes.
In this article, we highlight lessons from the RADx-UP Initiative to illustrate how equity-focused strategies can expand testing uptake today and in the future. These lessons provide a framework and important policy directions for scaling up community-based approaches. We provide a more in-depth description of the framework, barriers and challenges to community-based COVID-19 testing, and case examples and real-world solutions in a white paper by the RADx-UP Community Engagement core.
Five Policy Steps To Advance Health Equity
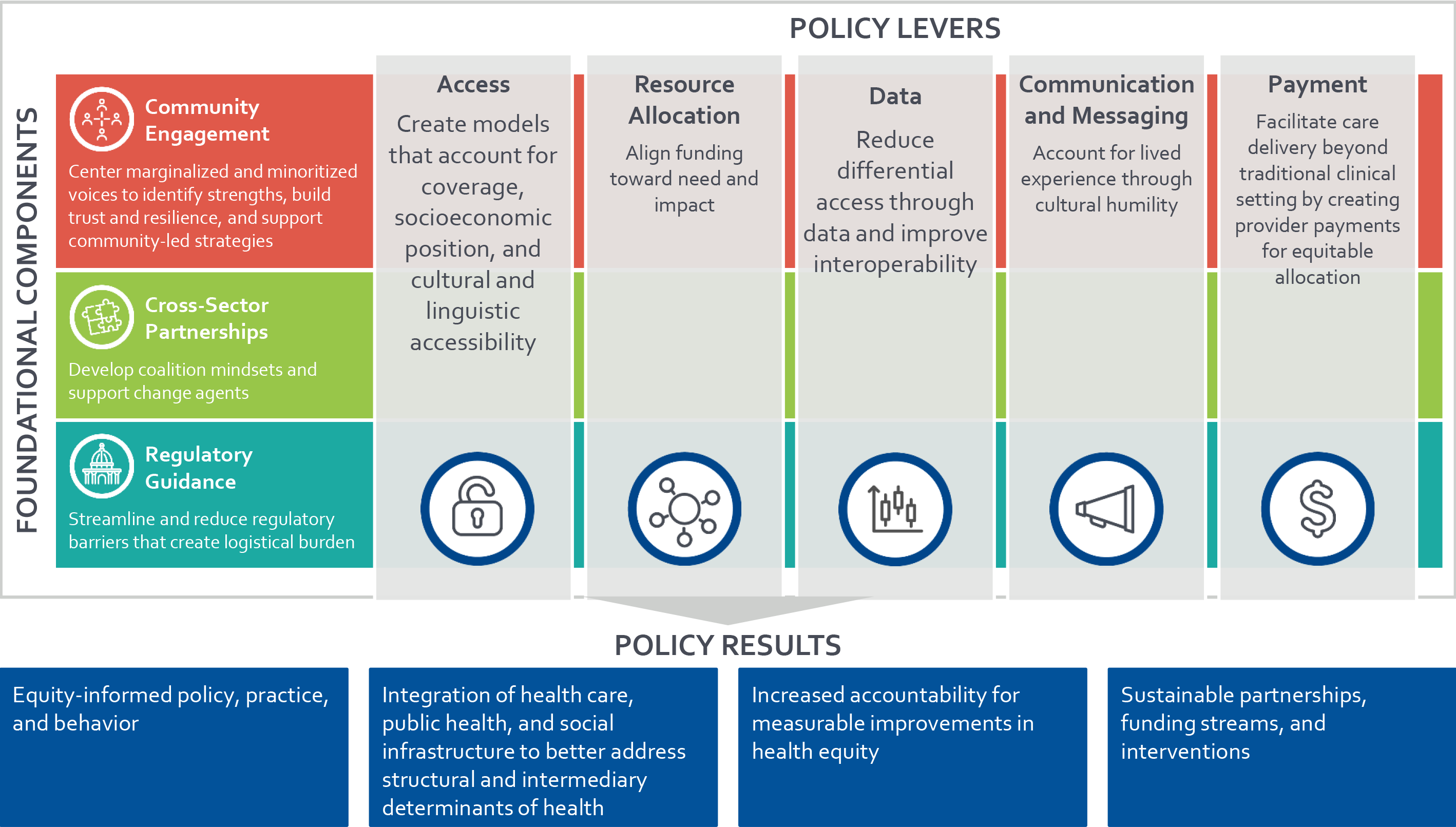
RADx-UP projects are focusing on increasing testing access and uptake for historically marginalized populations by implementing five key strategies: deploying mobile units to expand access, using disadvantage indices to prioritize resource redistribution, embedding community feedback into data collection, collaborating with community leaders to create key messages, and expanding provider payments to support community-based models.
Underlying these key strategies are foundational components including authentic community engagement research methods, developing cross-sector partnerships or coalitions, and streamlining regulatory guidance. Based on the experiences of RADx-UP research projects, we propose a framework for community-based testing that can be deployed today or in future COVID-19 surges (see exhibit 1).
Exhibit 1: Framework: community-based COVID-19 testing

Source: Authors’ analysis.
Develop Community-Based Strategies That Overcome Systemic Barriers To Increase Testing Access
Community-based strategies can bridge access gaps and deliver equitable testing by accounting for community assets such as existing infrastructure, established partnerships, community events, and gathering spaces. Often, these strategies extend services beyond the hospital, health system, or pharmacy setting in communities that experience lower access to pharmacies or historical and contemporary mistrust of the local health system. RADx-UP projects are improving the geographic availability of testing by establishing testing sites at schools, places of worship, local businesses, or deploying mobile testing vans. To further these efforts, policy makers should:
- Actively include community-based leaders in decision making as well as cross-sector partnerships with primary care settings or pharmacies.
- Extend health insurance coverage to address systemic inequities that underpin differential access to health services. While extending coverage is not a panacea to reducing health inequities, it is a first step to addressing coverage gaps among historically marginalized populations in the US.
- Collaborate with health systems, payers, and other health leaders to develop quality measures to capture the distribution of testing relative to the distribution of population or share of disease burden. These data can be used to develop and adapt plans to reach communities experiencing the greatest impact of COVID-19.
Use Disadvantage Indices Or Other Data Tools To Identify Communities To Prioritize For Resource Reallocation
Resource allocation efforts should center ethics, equity, and efficiency to maximize benefit and mitigate disparities. National and local data strategies to advance equitable resource allocation have included disadvantage indices, which rely on publicly available demographic and population-level data to help identify place-based social and environmental risk patterns.
Examples of disadvantage indices include the Centers for Disease Control and Prevention (CDC) Social Vulnerability (SVI) Index and the Area Deprivation Index (ADI), the Childhood Opportunity Index (COI), the NIH Pandemic Vulnerability Index (PVI), and the COVID-19 Community Vulnerability Index (CCVI). Each of these indices combine indicators across different social determinants of health to rank relative disadvantage by geographic area. RADx-UP projects are using disadvantage indices to pinpoint areas exhibiting the highest case rates and mortality to determine testing locations and intervention areas. To further these efforts, policy makers should:
- Use existing data (for example, electronic health records) to identify communities experiencing greatest vulnerability to direct resources.
- Allocate funding based on these data to support partnerships with federally qualified health centers and community health centers to expand prevention and treatment according to need.
- Create incentives for cross-sector data sharing to link case surveillance, hospital data, and other public health data for improved need identification.
- Consider different community contexts (for example, cultural, social, geographic, and economic) when assessing disadvantage indices to identify populations experiencing higher risk for other health conditions to more effectively designate services to historically marginalized populations.
Create Platforms For Community Feedback To Enhance Evidence-Informed Interventions And Strategies
Community engagement during data collection and reporting can facilitate trust, ensure sustainability of interventions, and address systemic deficits in data. These data gaps include missing race and ethnicity data, aggregated data that masks disparities, and misinformed classifications or categories. RADx-UP projects are working closely with community leaders, tribal nations, and organizations to identify testing disparities through data and to bring relevant data to community members through accessible platforms—such as advisory board meetings, town halls, and focus groups. To further these efforts, policy makers should:
- Develop funding mechanisms, such as grants, to support modernization of data management systems to meet real-time analysis demands—such as the CDC’s Data Modernization Initiative.
- Provide guidance on standards for data collection and reporting processes across sectors including sectors outside of the traditional health system.
- Design standardized, community-informed data formats, elements, and protocols to encourage data sharing and improve interoperability.
- Address privacy concerns related to extensive collection of data by increasing technical capacity to de-identify and anonymize data for data reporting.
- Consult with community members and boards when deciding on content and number of data elements to be collected to not inflict additional harm on communities.
Partner With Community Leaders To Develop Culturally And Linguistically Responsive Communication And Messaging
Community-based strategies can overcome systemic barriers by considering how different lived experiences, structural racism, and discrimination affect an individual’s access to and perception of health information. Many factors inform a person’s experiences and perceptions including their race or ethnicity, language, age, gender identity, sexual orientation, immigration status, housing status, disability status, political affiliation, or value system. RADx-UP projects are illustrating how public health communication and messaging must move beyond language translation to incorporate understanding of cultural nuances, values, beliefs, and systemic barriers. To further these efforts, policy makers should:
- Develop community advisory boards to provide perspectives on proposed public health decisions, policies, their impact, and the dissemination of information.
- Engage community leaders or coalitions to co-develop, review, and edit messaging before it is used in community settings.
- Support funding mechanisms for employing bilingual and bicultural staff to implement interventions in communities.
- Develop messaging in plain language and provide resources that address the needs of individuals with disabilities—such as communications in Braille and American Sign Language, or visual aids.
Expand Alternative Payment Models To Cover Community Health Workers Or Community-Based Organizations
Provider payment systems and policies influence how health care systems allocate resources and inform what services and care pathways are prioritized. Currently, health systems and states are experimenting with alternative payment models to create incentives to accelerate innovative care delivery models that advance health equity. Health equity is also a foundational pillar in new Centers for Medicare and Medicaid Services (CMS) initiatives including the Center for Medicare and Medicaid Innovation Strategic Refresh and recently announced Accountable Care Organization Realizing Equity, Access, and Community Health (ACO REACH) model.
As national and local payment reforms continue, officials should consider what additional steps can help align funding and incentives with interventions that address structural and social determinants of health. RADx-UP projects are demonstrating the importance of community health workers (CHWs) in connecting historically marginalized populations to necessary COVID-19 mitigation resources and supports. To further these efforts, policy makers should:
- Align financial incentives to expand and sustain care delivery models that reflect the critical role that CHWs and community organizations play as part of the care team.
- Encourage the development of equity-focused quality measures within value-based payment models to link equity to ongoing performance measurement.
- Create add-on or performance-based payments through new CMS initiatives, such as ACO REACH, and include payments for CHWs in Medicaid administrative cost claims to compensate CHWs and other community-based health care providers for their work delivered outside of traditional clinical settings (including time spent on community advisory boards).
- Develop long-term funding mechanisms for sustained community organization involvement in health promotion that move beyond the current research-dependent model.
- Build on lessons from the COVID-19 pandemic to extend services that mitigate health related social needs.
What’s Next?
As the pandemic response shifts from crisis intervention to reduced mitigation, policy makers must apply lessons learned to mitigate systemic inequities entrenched in processes, policies, and decision-making power. These inequities impact the health of all Americans. Lessons from RADx-UP projects demonstrate the feasibility of designing and scaling-up community-engaged COVID-19 testing models that prioritize the health and safety of historically marginalized populations while incorporating cultural humility and health justice.
RADx-UP projects represent substantial improvements in addressing continued systemic exclusion, medical mistrust, discrimination, systemic disenfranchisement, and structural racism in health care. Collectively, the RADx-UP projects offer a roadmap for implementing equity-focused strategies to overcome systemic inequities in both ongoing COVID-19 efforts and future public health or population health interventions.
Notably, the NIH built an infrastructure to support a network of academic-community partners through the RADx-UP initiative. This infrastructure can be expanded in the future to identify solutions that reduce disparities in all facets of population health. Based on these experiences, policy makers can more broadly adapt community-based approaches to meet other public health or population health needs.
Authors’ Note
The research on which this article is based was funded by the NIH RADx Underserved Populations (RADx-UP) Initiative (U24 MD016258).

[ad_2]
Source link


{kind=link}